Innovating with 3D Bioprinting in Microtia Surgery
Prof Mukherjee’s microtia program commenced in 2015. She leads the only cartilage bioprinting research program for microtia in Australia. Awarded >8M in research funding, this program fosters some of Australia’s brightest engineers and clinicians undertaking Mphil, PhD and post doctoral research.
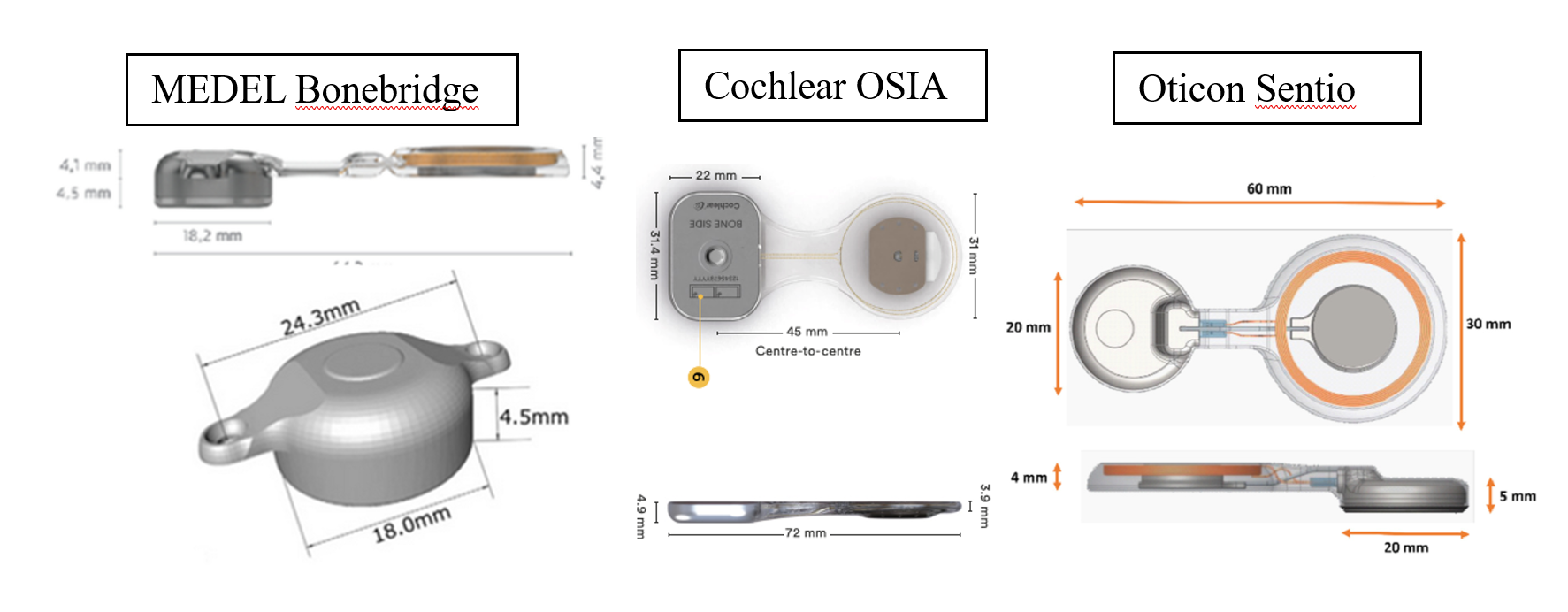
Prof. Mukherjee performs Australia’s First Paediatric OSIA Surgery
 Prof. Mukherjee performed Australia’s first paediatric OSIA surgery, which was also performed alongside 3D printed porous polyethylene implant performed by Dr Joe Dusseldorp and Dr Nicholas Lotz .
Prof. Mukherjee performed Australia’s first paediatric OSIA surgery, which was also performed alongside 3D printed porous polyethylene implant performed by Dr Joe Dusseldorp and Dr Nicholas Lotz .
About Microtia
The most common malformation (50%) affecting the head and neck, Microtia leaves patients deaf and with deformities impacting literacy and social development. The ear is divided into an outer, middle and inner ear. Microtia affects the development of the outer and middle ear structures. Surprisingly, the inner ear is seldom affected in Microtic patients unless the children have additional syndromes. This means that the most patients have a healthy cochlea and balance system. Hearing loss is usually mainly conductive in nature. If the conductive hearing loss is treated, then the patients often have very good perception of sound.
Microtia varies in severity from grade 1-4. Microtia can also be related to ear canal and middle ear abnormalities. If the ear canal is narrow but patent, there may be additional ossicular abnormalities (bones of the ear may be malformed) still creating a conductive hearing loss.
Grade 1: The ear is smaller than normal with minor abnormalities, but the key features of the normal ear are present.
Grade 2: Some of the features of the ear are missing, though usually much of the lower two-thirds of the ear is still present. The ear canal may be present, but frequently is very narrow (canal stenosis).
Grade 3: This is the most common type of microtia, in which the only feature remaining is a small peanut-shaped remnant ear lobe. The ear canal is usually completely absent (aural atresia). This will cause maximal conductive hearing loss in the affected ear.
Grade 4: Complete absence of the external ear without any remnant. This is called “anotia”, and is rarely seen.